





$21.97 on Amazon
Indians have high incidence of cardiovascular disease and stroke. This post discusses something that contributes to the risk for that – MTHFR mutations.
MTHFR is an enzyme involved in Vitamin B6 (and B12) metabolism.
There are mutations circulating that can reduce MTHFR enzyme activity.
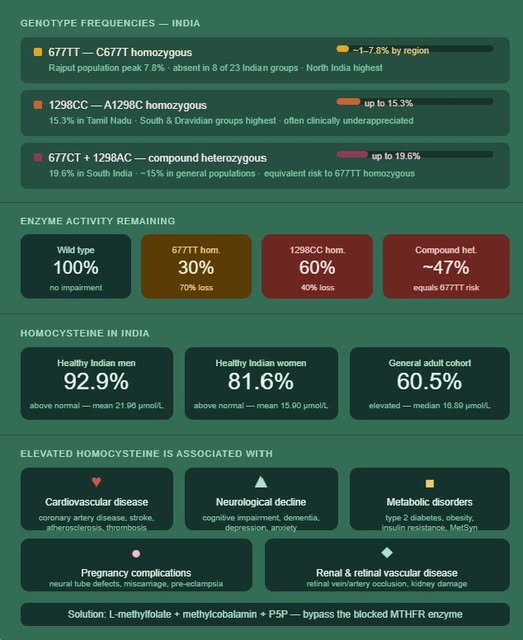
Wihout getting technical, about 20% of Indians are compound heterozygous for MTHFR mutations, and 7.8% are homozygous for the more damaging C677T mutation, resulting in about a 47-70% reduction in enzyme activity.
So basically, roughly up to 1 in 5 Indians can have impaired MTHFR enzyme activity thanks to thier genetics. If you have impaired activity, you need METHYLATED B vitamins, not the regular versions.
How does impairment manifest clinically? Through elevations of something called homocysteine.
Once we start looking at homocysteine elevation, the picture gets a LOT more dire (see image). There is astonishing, widespread elevation, at a degree that goes beyond just the genetic contribution. Diet can contribute. And maybe something beyond that. We just don’t know.
Homocysteine elevation is associated with cardiovascular diseases, including heart attacks, stroke, atherosclerosis, and venous blood clots. Earlier in life, in women, it can also be associated with pregnancy complications.
If you have the more deleterious MTHFR mutations and your doctor never brings it up (which I don’t think most do, in the absence of actual issues), you are not going to know until something bad happens: pregnancy complications, heart attacks, strokes.
Remember, 1 in 5 can have this issue. People are not going to find out when they are young. Testing for it is cumbersome, and in this day and age, I’m very hesitant to do a widespread genetic panel that puts my information out there. I found out I was MTHFR C677T heterozygous (so not the worst combination) after doing a panel for recurrent pregnancy loss. As I said, you usually don’t find out until something bad happens first.
If you are a person of Indian origin reading this, you have multiple options:
⇒ Hope you are one of the 4 out of 5 people who are fine, and go along your merry way
⇒ Blindly supplement with methylated B vitamins (likely does no harm)
⇒ Test homocysteine and/or test for MTHFR mutations
The other question is, if you are going to test or supplement, when will you do it? Are you interested in tackling the issue early, or do you want to wait until you see a problem? That, like everything else, is entirely up to you, in discussion with your doctor.
I’m C677T heterozygous, so my daughter has at least a 25% chance of having one copy of the C677T mutation. The other set of genes inherited is untested, so I don’t know her chances for the more problematic combinations. I could drag her in for testing, kicking and screaming. Or I could give her methylated B vitamins, and that’s the door I choose. You decide what’s right for you!
(not medical advice; this is purely an informational post)









